In the world of forensic pathology, few techniques carry as much historical weight and modern confusion as the Rokitansky method. You might assume the process of removing organs from a body follows a single, universal script, but the reality is far more complex. For decades, textbooks have debated whether the Rokitansky method involves removing organs one by one or keeping them connected. Some practitioners even mistake it for completely different procedures entirely. This confusion isn't just semantic; it changes how we understand death, disease, and safety in the autopsy suite.
Why does this specific method matter today? Because in an era where infectious diseases like COVID-19 remain a concern, knowing which procedure minimizes exposure to pathogens is critical. Furthermore, a landmark study published in late 2025 shed light on how the original technique had been misunderstood for over a century. Understanding the Rokitansky method means understanding the balance between preserving anatomical truth and protecting the pathologist performing the examination.
The Core Problem: Confusion Over Technique
If you pick up a forensic medicine textbook from ten years ago, you might find the definition of the Rokitansky method slightly blurry. Some authors described it as simply removing the organs in blocks. Others conflated it with the Letulle method, which removes everything in one single mass. This confusion stems from the evolution of medical terminology over the last two hundred years. While the name honors the Austrian giant Carl von Rokitansky, the exact mechanics of his "in situ" inspection often got lost in translation.
To clear this up, we have to look at what actually happens during a Rokitansky autopsy. Unlike the Virchow method, which dominates most modern hospitals, Rokitansky prioritizes looking at the organs while they are still inside the chest and abdominal cavities. Only after this thorough visual assessment does the actual removal begin. This subtle shift-from "remove then look" to "look then remove"-changes everything about how a pathologist interprets the case.
The Rokitansky Method is a specialized autopsy dissection technique characterized by systematic in situ examination of internal organs before their sequential en bloc removal. Named after Austrian pathologist Carl von Rokitansky, it emphasizes maintaining anatomical relationships between organs during the initial phase of the investigation. Originally designed in the mid-19th century, this approach was recently re-evaluated in the American Journal of Forensic Medicine and Pathology in 2025.
Anatomical Context: Why Position Matters
When you remove an organ immediately after opening the body, you lose its context. Think of pulling a plant out of the ground to examine its roots. If you pull it straight out, you snap the root system. You see the parts, but you miss how those parts were anchored and connected to the soil. In human anatomy, organs don't just sit next to each other; they share blood vessels, nerves, and ducts.
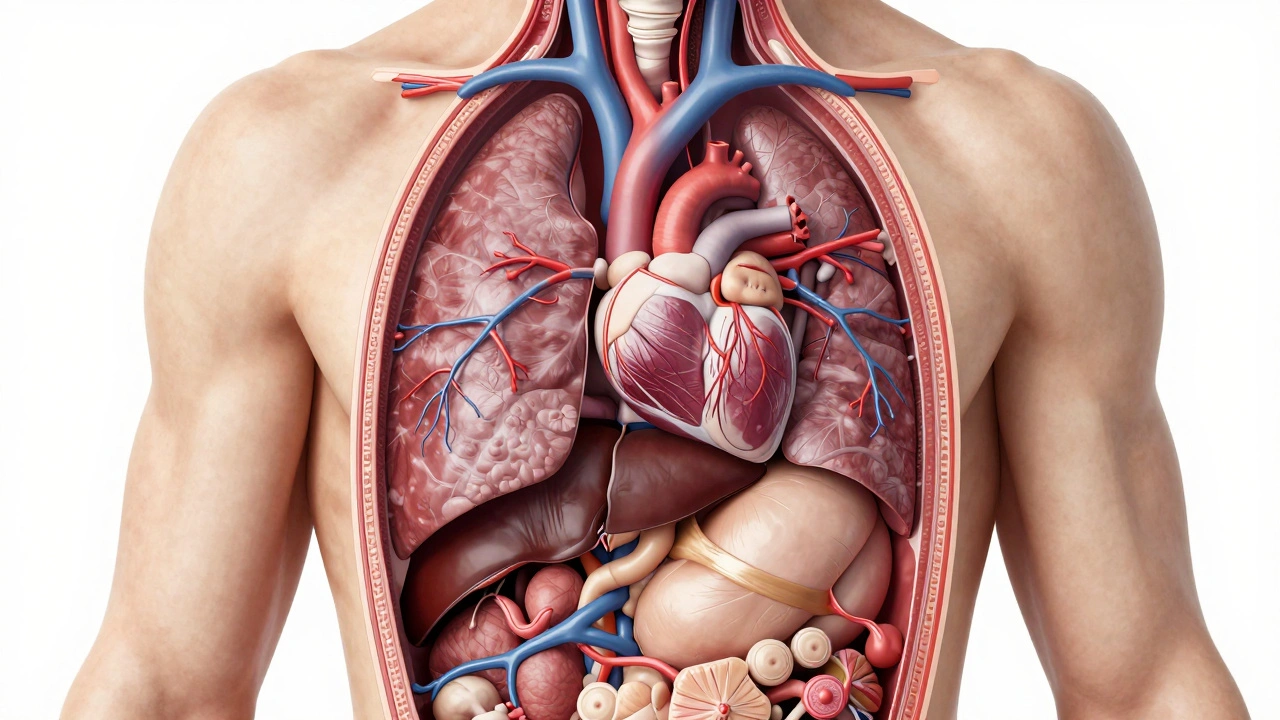
The Rokitansky technique keeps this "soil connection" intact longer. By inspecting the liver, spleen, and kidneys while they sit in their natural beds within the thoracic and abdominal cavities, a pathologist can spot abnormalities that might be missed once the tissue is cut away. Color changes in the surrounding tissue, fluid accumulation, or unusual adhesions between organs become visible clues only preserved when the organ stays in place until examined.
This focus on position is crucial for diagnosing systemic issues. If a disease affects multiple systems-like heart failure causing congestion in the lungs and liver-the Rokitansky method allows the examiner to see the spatial relationship of that congestion across different structures without disrupting the vascular connections prematurely.
Step-by-Step: Executing the Protocol
Performing a Rokitansky-style evisceration requires discipline and a specific sequence of cuts. It is not a hurried process. Here is how a trained forensic professional typically navigates this procedure:
- Initial Incision and Reflection: The surgeon makes the Y-incision and reflects the skin and chest wall flaps. At this stage, nothing is removed. The focus is purely on observation.
- In Situ Inspection (Thorax): The pathologist inspects the lungs and heart within the cavity. They check for trauma, hemorrhage, or discoloration before severing major vessels. This preserves the state of the cardiovascular system relative to the lung tissue.
- In Situ Inspection (Abdomen): Moving downward, the abdominal organs are exposed. The liver, stomach, intestines, and spleen are visually assessed. Texture, color, and positional shifts are noted without lifting the organs out of the peritoneum yet.
- Sequential Removal: After documentation, removal happens. Crucially, Rokitansky did not remove organs individually like the Virchow method. Instead, he utilized a block approach. The abdominal viscera might be removed as a connected unit to preserve the hepatobiliary tract connections.
- Post-Removal Dissection: Once the block is out, detailed internal cutting occurs on the bench. But the critical data gathering happened inside the body first.
This workflow distinguishes itself from the rapid "grab-and-go" approach of some emergency autopsies where speed is the primary goal. It trades time for accuracy in anatomical preservation.
Comparative Analysis: Rokitansky vs. Virchow vs. Letulle
You cannot fully grasp the Rokitansky method without comparing it to its neighbors in the autopsy suite. The landscape of dissection techniques is defined by three main players, each solving a different problem for the forensic investigator. Below is a breakdown of how they compare regarding their core philosophy and application.
| Method | Primary Approach | Organ Connection | Best Use Case |
|---|---|---|---|
| Rokitansky | In situ inspection before removal | En bloc (block removal) | Anatomical preservation, infectious risk |
| Virchow | One-by-one organ removal | Dissociated (severed) | Standard hospital autopsies, common causes of death |
| Letulle | Mono-block removal | Entire block as one unit | Rapid decomposition scenarios |
| Ghon | Group block removal | Three separate blocks | Trauma-focused cases |
Note the distinct difference in the "Organ Connection" column. The Virchow method is excellent for routine cases where you want to isolate specific organs for toxicology without worrying about systemic layout. However, it breaks the "map" of the body. The Letulle method moves faster but treats the viscera almost like a single lump. Rokitansky sits in the middle, offering the map (context) while allowing for structured removal.
Safety First: Application in Infectious Disease
The most compelling reason to reach for the Rokitansky protocol today involves occupational safety. We live in a post-pandemic world where biological hazards are a constant reality in the morgue. When dealing with bodies from patients who died of high-risk communicable diseases, minimizing aerosolization and spillage is not optional-it is mandatory.
The Rokitansky method excels here because of the "organ retention" principle. By keeping organs inside the body cavity for the duration of the initial examination, you reduce the surface area of tissue exposed to the room air. There is less handling of individual organs, which reduces the chance of a needle stick, a slip with a scalpel, or a splash of contaminated fluid onto the technician's face shield.
Infectious Disease Autopsy is a specialized procedure conducted on deceased individuals known or suspected to have communicable conditions such as HIV, Hepatitis C, or viral respiratory infections. These protocols prioritize the safety of forensic staff through techniques like limited evisceration and enhanced PPE usage. The Rokitansky method supports this by reducing organ handling.
Recent guidelines have reinforced the use of this technique for HIV-positive decedents or those with active tuberculosis. The method allows the pathologist to gather necessary visual data without creating a high-risk environment. If the organs remain covered by the body's own walls for longer, the external threat level drops significantly.
The 2025 Rediscovery: Correcting the Record
There is a fascinating twist in the academic narrative of this technique. For nearly one hundred years, English-language literature suffered from nomenclature drift. Many texts began referring to the "en masse" removal of organs (typically associated with Letulle) as the Rokitansky method. This conflation caused significant friction in training programs. Students were taught one method, called it Rokitansky, but were actually practicing something else entirely.
This changed dramatically in September 2025. A publication titled "The Rokitansky Autopsy Method, Rediscovered" appeared in the American Journal of Forensic Medicine and Pathology. The authors conducted a deep dive into the original German manuscripts of Carl von Rokitansky. They discovered that his true method was never lost, but rather obscured by misattribution. The article argued that the modern understanding of the technique had been simplified too much, losing the nuance of the "inspection before removal" rule.
This correction matters because it restores the integrity of the procedure. By acknowledging the true steps-inspect in situ, then remove en bloc-we can appreciate why Rokitansky remains a vital tool in the forensic arsenal. It wasn't just about speed; it was about precision. That precision becomes the difference between a correct diagnosis of a systemic disease and a missed finding.

Common Pitfalls and Misconceptions
Even experienced examiners stumble over the specifics of Rokitansky dissection. One common error is rushing the inspection phase. The value of the method relies on the time spent looking at organs in the cavity. If a practitioner skips this step and immediately begins dissecting connections, they revert to a hybrid Virchow style, negating the benefits of anatomical context.
Another misconception is assuming the method is "old-fashioned." While Virchow is standard for general medicine, Rokitansky finds its niche in complex pathology and forensics. Trauma reconstruction, particularly involving the torso, benefits immensely from seeing exactly how blood vessels were torn relative to their neighbors. Ignoring the anatomical context can lead to reconstructive errors in determining the trajectory of a wound.
Finally, confusion regarding the "Rokitansky-Aschoff sinuses" or specific anatomical landmarks named after him often bleeds into procedural discussions. Students must distinguish between the pathologist's legacy of anatomical naming versus the autopsy technique itself. Keeping these distinct helps maintain clarity during medical board examinations.
Next Steps for Practitioners and Students
For those studying forensic medicine, integrating the Rokitansky method into your mental model is essential. Do not dismiss it as obsolete theory. Instead, view it as the safety-first alternative for high-hazard autopsies and the context-rich alternative for complex systemic pathology. When you encounter a case file mentioning "organ block removal," pause and ask if the in situ inspection was documented. If not, consider that critical evidence may have been lost.
Training centers now emphasize this distinction. Simulation labs are incorporating modules that require trainees to perform a dry run of the in situ inspection checklist before touching the removal knives. This builds muscle memory for the safety advantages. As we move further into 2026, expect to see more digital documentation of the "in situ" phase, ensuring that the anatomical relationships are captured digitally even if physical connections are severed later.
Frequently Asked Questions
Is the Rokitansky method still used in 2026?
Yes, though it is less common than the Virchow method for routine cases. It is frequently chosen for infectious disease autopsies, traumatic deaths, and complex systemic disease investigations where anatomical relationships must be preserved.
What is the main advantage of the Rokitansky method?
Its primary advantage is the ability to preserve anatomical relationships between organs. By examining organs in situ before removal, pathologists can better understand how diseases affect interconnected systems without disrupting the natural positioning.
How does Rokitansky differ from Letulle?
While both involve block removal, Letulle removes the entire visceral mass in one piece quickly, whereas Rokitansky emphasizes a detailed examination of the organs inside the body cavity prior to any extraction.
Why is the Rokitansky method good for infectious diseases?
Keeping organs inside the body cavity during the initial inspection minimizes exposure to pathogens. It reduces the handling of tissue, lowers the risk of spillage, and protects the forensic team from direct contact with hazardous fluids.
Did Carl von Rokitansky invent the autopsy?
No, he did not invent the autopsy. However, he revolutionized the *methodology*. He introduced systematic clinical-pathological correlation and specific dissection sequences that laid the groundwork for modern forensic pathology.
What caused the confusion around the method in recent decades?
Over time, the term became loosely applied to various en bloc techniques. This nomenclature drift was clarified by a 2025 study that traced Rokitansky's original instructions back to their source material.
Can you use Rokitansky for a standard heart attack case?
It is possible, but inefficient. For straightforward heart attacks, the Virchow method is faster and sufficient. Rokitansky is best reserved for complex systemic issues or safety-critical scenarios.