When a bullet strikes the body, it doesn't just create a hole. It transfers kinetic energy, shatters bone, and creates invisible shockwaves that tear tissue far beyond the bullet's actual path. Understanding this damage is not just about medicine; it is the core of gunshot wound analysis, a discipline where forensic pathology meets physics to reconstruct violent events. For investigators, pathologists, and trauma surgeons, reading these injuries correctly can mean the difference between solving a homicide and failing justice, or saving a life in an emergency room.
This guide breaks down how experts analyze firearm injuries. We will look at the science of wound ballistics, which explains how projectiles interact with human tissue, how to distinguish entry from exit wounds, and how modern imaging changes the game. Whether you are studying forensics or working in law enforcement, understanding these patterns is essential.
The Science of Wound Ballistics
To understand a gunshot wound, you first need to understand the energy behind it. This field relies on three types of ballistics. Internal ballistics covers what happens inside the gun when the trigger is pulled. External ballistics tracks the bullet through the air. But for us, the most important is terminal ballistics, also known as wound ballistics, which studies the interaction between the projectile and the target tissue.
Think of a bullet like a car crash. The damage depends on speed and weight. A small, slow bullet causes less damage than a heavy, fast one. The formula for kinetic energy is E = ½mv². Because velocity (v) is squared, doubling the speed quadruples the energy.
- Handgun rounds: A typical 9mm bullet travels at about 360 meters per second. It carries roughly 260 Joules of energy. This usually creates a narrow track.
- Rifle rounds: A 5.56mm rifle bullet can travel at 900 meters per second. That same weight now carries over 1,600 Joules-more than six times the energy of the handgun round.
This massive difference in energy changes everything. High-velocity rifle bullets often fragment or tumble inside the body, creating large, irregular cavities. Handgun bullets tend to stay intact, leaving a more predictable path. Knowing the weapon type helps predict the injury pattern before you even see the X-ray.
Permanent vs. Temporary Cavitation
One of the biggest myths in popular culture is the idea of "hydrostatic shock" causing instant incapacitation from pressure waves alone. Research by Martin Fackler at the U.S. Army Wound Ballistics Laboratory debunked this. He showed that real damage comes from two sources: permanent cavity and temporary cavity.
Permanent cavity is the actual hole left by the bullet. It consists of crushed and torn tissue along the bullet’s path. In soft tissue, this hole is usually only slightly wider than the bullet itself. If the bullet hits bone, fragments act like secondary missiles, shredding nearby organs and nerves. This crushing effect is what kills or disables.
Temporary cavity is the stretch of tissue pushed aside by the bullet's energy. Imagine throwing a stone into water; the water bulges out before settling back. In high-energy rifle wounds, this temporary cavity can expand to 13 times the bullet's diameter. However, elastic tissues like lungs snap back quickly and may survive. Non-elastic tissues like the liver or brain do not bounce back well and suffer severe damage from this stretching. Most handgun wounds do not generate enough energy to cause significant temporary cavitation damage in elastic organs.
Identifying Entry and Exit Wounds
Determining the direction of fire is critical for reconstruction. You cannot simply guess based on size. A small exit wound might be smaller than a large entry wound if the skin was supported by a wall or tight clothing-a phenomenon called a "shored" wound. Instead, look for specific features.
| Feature | Entry Wound | Exit Wound |
|---|---|---|
| Abrasion Collar | Present (1-3 mm wide ring of abraded skin) | Absent |
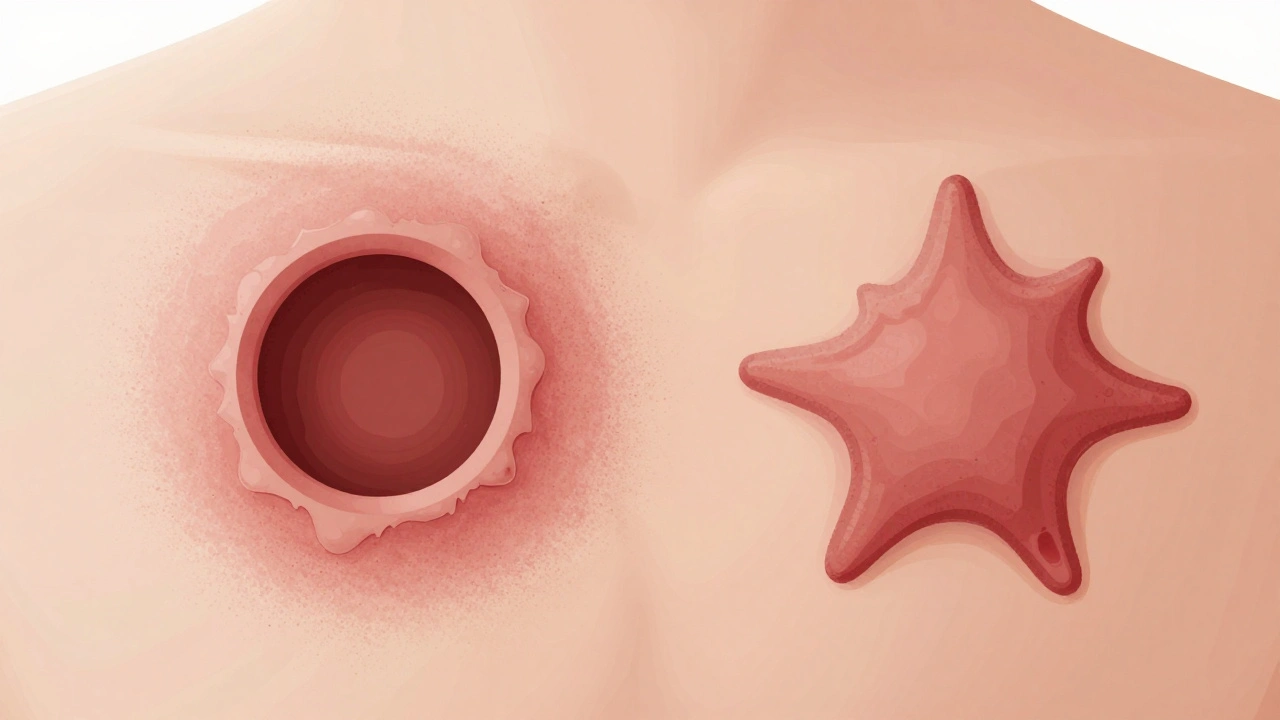
| Shape | Usually circular or oval; may be smaller than bullet due to skin elasticity | Irregular, stellate (star-shaped), or slit-like; often larger than entry |
| Edges | Inverted (rolled inward) | Everted (rolled outward) |
| Contamination | Soot, powder stippling, or muzzle imprint (depending on range) | Clean margins, no soot or powder |
| Bone Beveling (Skull) | Internal beveling (cone shape points inward) | External beveling (cone shape points outward) |
In skull fractures, the bone tells a clear story. When a bullet enters the skull, it punches inward, creating a cone of broken bone that is narrower on the outside and wider on the inside. At the exit site, the bone bursts outward, creating the opposite pattern. Radiologists use CT scans to spot this internal vs. external beveling instantly.
Estimating Range of Fire
How close was the shooter? Forensic pathologists categorize distance into four groups based on residue found on the skin. These deposits come from unburnt gunpowder, smoke, and gases expelled from the barrel.
- Contact Wounds: The muzzle touches the skin. You will see a distinct muzzle imprint burned into the skin. In head shots, gas expands inside the skull, causing the scalp to tear into a star shape. Blood and tissue may be blown back into the barrel.
- Near-Contact Wounds: Within a few centimeters. Heavy soot deposition and searing of the skin occur, but there is no clear muzzle imprint.
- Intermediate Range: Typically from a few inches up to 60-90 cm (depending on the ammo). The key sign here is stippling or tattooing. Unburnt powder grains hit the skin like tiny pellets, leaving red or black dots. They do not penetrate deeply but stain the epidermis. Washing the area removes soot but not stippling.
- Distant Range: Beyond the reach of powder and soot. The wound looks clean, with only the abrasion collar visible. No residue is present.
Remember, exact distances vary wildly by firearm. A revolver might deposit stippling at 90 cm, while a semi-automatic pistol might stop at 45 cm. Forensic reports usually state ranges as "consistent with less than X cm" rather than giving a precise number, unless test-firing with the exact weapon confirms it.
Trajectory and Imaging Technology
Reconstructing the bullet's path helps place the shooter and victim in space. In living patients, CT scans and CT angiography (CTA) are the gold standard. A study by Kauvar et al. found that CT has over 95% sensitivity for detecting bullet trajectories and associated organ damage in torso trauma.
On imaging, a wound track appears as a linear distribution of gas, hemorrhage, and metal fragments. Directionality clues include the angle of bone fragments and the bevelling mentioned earlier. However, caution is needed. Bullets deflect off bone, and bodies move after death. A straight line drawn from entry to exit on a static body might not reflect the true path if the victim fell or twisted during the shooting.
In forensic autopsies, pathologists use trajectory rods to map the path. They correlate this with scene measurements. Modern techniques like post-mortem CT (PMCT) allow for 3D reconstructions of the entire body, identifying fragments missed by traditional dissection. This virtual autopsy approach is becoming standard in many European and North American centers.

Regional Injury Patterns and Mortality
Where the bullet hits matters more than the caliber. Different body regions have different survival rates.
- Head: Highest mortality. Civilian cranial gunshot wounds have mortality rates between 64% and 90%. Survival depends heavily on the initial Glasgow Coma Scale (GCS) score. Patients with a GCS of 3-5 rarely survive, while those with 9-15 have a better than 70% chance.
- Chest: Often involves lungs, heart, or major vessels. Overall mortality is around 10%, but it jumps to over 50% if the heart or aorta is hit. Rapid decompression of tension pneumothorax (air trapped in the chest cavity) is a common immediate killer.
- Abdomen: Usually requires surgery (laparotomy). Damage control surgery focuses on stopping bleeding and controlling contamination first, with definitive repairs done later once the patient is stable.
- Extremities: Least lethal but high risk for long-term disability. About 9% involve vascular injury and 8% involve nerve damage. Limb-threatening ischemia occurs in 3-4% of cases.
Shotgun wounds add another layer of complexity. At close range (<60-90 cm), the shot acts like a single solid slug, creating a massive defect. At longer ranges, the pellets spread out. A common rule of thumb is one inch of spread per yard, but this varies by choke and load. Close-range shotgun wounds often mimic contact gunshot wounds with severe tissue destruction.
Medicolegal and Public Health Context
Guns don't just leave physical marks; they leave data trails. The CDC updated its surveillance definition for firearm-related injuries in 2025. Now, any case presenting for medical care, appearing in EMS records, or listed in vital records with a firearm injury code counts. This broad definition captures the full scope of the crisis.
In the U.S., firearm deaths exceeded motor vehicle deaths for children and adolescents in 2020. With nearly 49,000 firearm deaths annually, the public health burden is immense. Nonfatal injuries are even more common, with estimates suggesting two nonfatal ED visits for every fatal shooting. This means hundreds of thousands of people live with the chronic pain, PTSD, and functional impairment described in studies by Richmond et al., where over 50% of survivors developed probable PTSD within six months.
For legal cases, determining manner of death (homicide, suicide, accident, or undetermined) relies on combining wound analysis with scene evidence. Bagging hands to preserve gunshot residue (GSR) in potential suicides, documenting the position of the body, and collecting trace materials before moving the victim are crucial steps emphasized in training manuals like those from the Idaho Sheriffs’ Association.
What is the difference between a penetrating and a perforating gunshot wound?
A penetrating wound has an entry point but no exit; the bullet remains inside the body. A perforating wound has both an entry and an exit point, meaning the bullet passed completely through the body. Perforating wounds generally cause more extensive tissue damage due to the longer path and higher energy transfer required to exit.
Can you determine the caliber of a bullet from the size of the entry wound?
No, not reliably. Skin is elastic and often stretches then snaps back, making the entry wound smaller than the actual bullet diameter. Additionally, clothing can distort the wound shape. Forensic experts rely on recovered bullets, shell casings, and ballistic testing rather than wound size alone to determine caliber.
What is stippling in a gunshot wound?
Stippling, also called tattooing, consists of tiny puncture marks caused by unburnt gunpowder grains hitting the skin. It indicates an intermediate range of fire, typically between a few inches and several feet, depending on the firearm and ammunition. Unlike soot, which washes away, stippling embeds in the skin and is permanent.
Why do high-velocity rifle wounds cause more damage than handgun wounds?
Rifle bullets travel much faster (850-950 m/s vs. 330-400 m/s for handguns), resulting in significantly higher kinetic energy. This energy creates a large temporary cavity that stretches and tears tissue far beyond the bullet's path. Rifle bullets also tend to fragment or yaw (tumble) inside the body, increasing the surface area of damage and creating irregular, large permanent cavities.
How does bone beveling help identify entry and exit wounds in the skull?
When a bullet enters the skull, it pushes bone inward, creating a fracture cone that is narrower on the outside and wider on the inside (internal beveling). When it exits, the bone bursts outward, creating a cone that is wider on the outside and narrower on the inside (external beveling). CT scans clearly show these patterns, allowing radiologists to determine the direction of travel.